Children and young people who have experienced social care interventions are often rejected by Child and Adolescent Mental Health Services (CAMHS) due to the same factors that may be contributing to their poor mental health, according to analysis of case notes.
In 2024, findings from the COACHES project documented that children and young people with social care involvement were three times more likely to be rejected by CAMHS. A year later, further research funded by the National Institute for Health and Care Research (NIHR) shed light on the reasons why children with some of the highest levels of need are being rejected for mental health support.
Professionals often cited “social factors” like an unstable home environment, insecure legal status, poor social conduct and relationships – which can all cause anxiety, depression and poor mental health - for justifying rejection. They claimed that the young person’s needs were due to their “social” context, rather than “medical” or “psychological” issues. It appeared that professionals felt that “social stability” was needed for young people to be accepted by CAMHS, but it was unclear what “social stability” meant and the term was applied inconsistently across cases.
Read our policy briefing on the findings of this latest COACHES study
The analysis of case notes, examining over 20,000 case notes relating to 70 people, was conducted by a team of researchers and people with lived experience of children’s social care and mental health services.
COACHES is a collaboration between the University of Cambridge, Kingston University, King’s College London, NCB, the British Association of Social Workers and the Care Leavers Association.

The case notes cover the years following austerity measures and include the COVID-19 pandemic and lockdowns. The research found that, with limited resources, “complex” or resource-intensive cases tended to be rejected, and that services tended to approach mental health from a biological, diagnostic-led perspective rather than taking social factors such as family circumstances, bullying, or immigration status into account. When signposted to other services, young people often returned to CAMHS with escalating needs, indicating that lower-level interventions were insufficient to support their mental health needs.
The findings of this study align with other research indicating that public resources are failing to go into supportive help for children and families, and instead are forced into late-stage crisis interventions*. This is in line with council spending on children’s social care services, where residential care spending surpassed early help for the first time last year.
The paper’s authors called for:
- A review of CAMHS referral criteria for children and young people with social work involvement.
- Increased investment in CAMHS with a long-term funding model and distribution plan.
In May 2025, a consensus report, led by UK Trauma Council, University College London, and partners, was launched, titled: Increasing access to evidence-informed mental health service provision for children in care in England: National Recommendations for Change.
The COACHES study lead was invited to join this group of leading academic and clinical experts to develop these collaborative national recommendations on improving evidence-informed mental health provision for care-experienced young people. This work was led by the UK Trauma Council and University College London, with support from CoramBAAF, NCB and other partners. Recommendations span commissioning, cross-sector workforce training, service integration, and referral and clinical decision-making. The report is specific to care-experienced young people, but likely more broadly applicable to children with a social worker.
The report calls upon the Department of Health and Social Care and Department for Education to:
- Pilot an integrated mental health service, that brings together relevant children’s social care and NHS mental health staff in a co-located service under a pooled-budget: to increase the accessibility of mental health support, shared-decision making and referral processes, and deliver evidence-based direct and indirect mental health interventions to this population.
- Require children’s social care and CAMHS leadership, along with other key stakeholders, to develop shared service delivery plans, to ensure all parties have a clear and agreed understanding of the mental health provision available in the area to this population of young people, and gaps in that provision.
- Develop a new children’s social care mental health practitioner training programme to ensure the children’s social care based mental health workforce is trained and supported to deliver evidence-based trauma-informed therapies to these young people, whilst also providing important professional development opportunities. This could be modelled from the NHS-E funded Education Mental Health Practitioner training programme and support the co-located model of practice.
For more information about this report and the full list of recommendations see UK Trauma Council.
*Hood, R., Gorin, S., Goldacre, A., Muleya, W., & Bywaters, P. (2020). Exploring drivers of demand for child protection services in an English local authority. Child & Family Social Work, 25(3), 657-664
We are experiencing a mental health epidemic which feels especially cruel to children and young people. Whether it’s cuts to funding and austerity decisions, burnt-out workforce, and long waiting lists with no access to life-saving care, we are failing the most vulnerable children and young people and sending them off into the world with two broken legs, expecting them to place first in the London marathon. It should be a moral duty, an act of humanity and a collective effort to fight for better care and services for children and young people suffering with their mental health.
Jack Smith
Co-author with lived experience of children's social care and mental health services

About NIHR
The mission of the National Institute for Health and Care Research (NIHR) is to improve the health and wealth of the nation through research.
We do this by:
- funding high quality, timely research that benefits the NHS, public health and social care
- investing in world-class expertise, facilities and a skilled delivery workforce to translate discoveries into improved treatments and services
- partnering with patients, service users, carers and communities, improving the relevance, quality and impact of our research
- attracting, training and supporting the best researchers to tackle complex health and social care challenges
- collaborating with other public funders, charities and industry to help shape a cohesive and globally competitive research system
- funding applied global health research and training to meet the needs of the poorest people in low and middle income countries
NIHR is funded by the Department of Health and Social Care.
Our work in low and middle income countries is principally funded through UK international development funding from the UK government.
The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
About the research
Morgan, T. et al (2025) “The social must be stabilised: How are the social needs of young people with social work involvement characterized in their mental health case notes?” Social Science and Medicine 374. https://doi.org/10.1016/j.socscimed.2025.118052
This research is part of the NIHR-funded COACHES project, a collaboration between the University of Cambridge, Kingston University, King’s College London, NCB, the British Association of Social Workers (BASW) and the Care Leavers Association examining data from over 100,000 young people across two NHS trusts.
Case notes were sourced from the Clinical Record Interactive Search (CRIS) dataset based in the South London and Maudsley (SLAM) NHS trust. Half of the young people accepted by this NHS Trust have identified safeguarding needs and a fifth have social care involvement (Coughlan et al., 2024). This project has been approved for secondary data analysis by the University of Oxford (23/SC/0257). All patients have consented for their anonymised notes to be used for research purposes. These notes include unstructured fields, referral documents, correspondence, progress notes and demographic data. These case notes are principally produced by CAMHS professionals but also include notes from G.Ps., A&E doctors, educators, social workers, police officers, and occasionally young people and their guardians. Case notes span from 2007 to present, capturing a period slightly before the introduction of austerity measures following the 2008 global financial crisis. They also include information from the COVID-19 pandemic where services had to shift almost exclusively to online consultations. One analyst, guided by conversations with the wider Expert by Experience team, selected 70 cases which aimed to reflect the diversity of the sample by including a variety of genders, ages, ethnicities, mental health diagnoses and difficulties, and levels of social work involvement. The 70 cases included 20,166 unique case notes. Young people had between 33 and 2672 case notes (mean =288).
Findings
- Young people whose emotional distress or behavioural challenges were identified as principally relating to “social” or “contextual” stressors almost always had their CAMHS referral rejected.
- Acute “contextual” crises, including the legal ramifications of physical and sexual abuse, had to be resolved for CAMHS to accept a young person into the service.
- When young people’s needs were deemed as “too chaotic”, their request was often rejected or treatment was stopped.
- Young people’s social needs were often only accepted by the service where they were viewed as elevating the risk of clearly diagnosable psychological or neurological conditions.
- When possible, CAMHS outsourced treatment by signposting young people with “social” needs to other services, such as charities or the young person’s school.
- When young people presented risks “too great to manage in the community”, they were often sectioned within in-patient facilities and their liberty was restricted. This often happened when young people had previous unaddressed, long-standing social and mental health needs.
- When rejected, the responsibility of care often fell to families and the young people themselves. This often resulted in readmissions to A&E for suicide or self-harm.
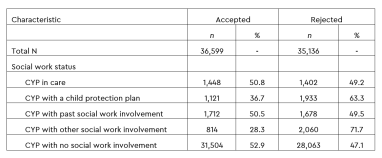
Previous studies show that children and young people with experience of social work are up to four times more likely to suffer from a mental health condition (a). A different study suggests that up to half of children and young people in care suffer from a mental health condition. (b) This suggests that, although the rates of rejection between children with and without social work involvement are similar, the unmet need among children with social work involvement is much higher than their peers.
(a) Ford T, Vostanis P, Meltzer H and Goodman R (2007) Psychiatric disorder among British children looked after by local authorities: Comparison with children living in private households. British Journal of Psychiatry 190(4), 319-325. https://doi.org/10.1192/bjp.bp.106.025023
(b) Bronsard G, Alessandrini M, Fond G, Loundou A, Auquier P, Tordjman S and Boyer L (2016) The prevalence of mental disorders among children and adolescents in the child welfare system: a systematic review and meta-analysis. Medicine 95(7), e2622. https://doi.org/10.1097/MD.0000000000002622
Case notes extracts (names have been changed)
Rejected because of their “social situation”
- Alex, a 12-year-old was brought into A&E after having taken a suspected overdose and running away from their new foster placement which they had recently shifted to due to “complex family dynamics.” Nevertheless, because their presentation was deemed “substantially social” they were rejected by mental health services on the basis that they “need [social service] intervention and generic support with emotional regulation” (33HSWOWB).
- Benedict, a 16-year-old unaccompanied asylum seeker was rejected from CAMHS on the basis that “Although he was expressing distress, it was primarily in the context of him being very unhappy in his foster placement” (34HSWMBB).
- “Coulson does not meet the criteria for a moderate to severe mental health difficulty and initial assessments around possible underlying neurodevelopmental difficulties have been inconclusive…Coulson’s lack of contact from his father and bereavement of his grandmother may be predisposing factors to his emotional dysregulation” (12HSWMWB)
- A 10-year-old boy's CAMHS assessment mentioned a history of self-harm, restrictive eating, hearing voices, and aggression to others. Nevertheless, because his difficulties were located with mother's cultural difficulties of accepting his sexuality, he was deemed to not have “any significant mental health issues”. This assessment was also made on the basis that he was also already engaged with a counselling charity and his CAMHS case was closed (2LSWMB)
- Rejected because of unresolved acute crisis (sexual violence)
- “CAMHS would not be able to act in this matter until it is clear that safeguarding issues are dealt with, and the [sexual abuse] allegations have been properly investigated” (29HSWO; 1LSWFMR)
- Rejected because lacking a “stable base” or “too chaotic”
- “Gwen has been open to [the service] since her referral in 2018, she has not had the opportunity to experience a stable placement on a consistent basis… Gwen has not been in a settled enough placement to allow her to engage in any therapeutic process” (06HSWFMR)
- Direct therapy was stopped for a family on the basis that mum would not have capacity as “things might be a bit too chaotic at the moment” (31HSWOWB)
- Accepted, but “social needs” remained secondary
- Peter, a 13-year-old boy was deemed to meet psychological criteria of “depressive illness in the context of social stressors”. This is because his bullying was connected to his onset of seeing visions and hearing voices, and persistent “suicidal thoughts by hanging”. Nevertheless, because a CAMHS assessment determined that “as risk is low and difficulties indicated as mild-moderate in range, consider for Tier 2 services. brief intervention… possibly by trainee psychologist.” (32LSWMWB).
- Outsourcing support or treatment
- “Following CAMHS extended assessment, evidence was not conclusive to warrant a diagnosis of ADHD. Instead specific recommendations have been made for school around exploring specific learning difficulties and working with SENCO” (32LSWMWB)